How is MDI (Multidirectional Instability)
treated?
The treatment for MDI must be individualized for each patient.
Non-Operative Treatment
Most patients with MDI can be treated non-operatively with a physical
therapy program that emphasizes muscular rehabilitation. Rehabilitation
focuses on strengthening the rotator cuff muscles and
periscapular muscles (those around the scapula). Strengthening
these muscles provides dynamic stability to the joint, which is especially
important when the static stability provided by the ligaments is lacking.
The vast majority of patients (about 90%) who follow a rehabilitation
program diligently for at least six months will achieve pain relief.
Those who continue with a daily or weekly exercise program as outlined
by the doctor are most likely to have a successful recovery.
Athletes may also benefit from sport-specific rehabilitation
that includes technique evaluation and modification. Often this type
of program can help eliminate faulty technique that may have led to
the development of symptoms.
Patients who do not get relief from symptoms with a physical therapy
program are a treatment challenge. Only about 70-80% of these patients
eventually achieve long-term stability, with 60-70% reaching the level
of athletic participation they enjoyed prior to the instability.
Operative Treatment
The most challenging patient to treat surgically is the athlete whose
symptoms continue following a rehabilitation program. Often athletes
are successful in their sport because of increased laxity in the joint;
so surgical intervention should only be considered when the patient
has a thorough understanding of MDI, and is aware that stability with
surgical correction is always achieved at the expense of motion. Patients
who can voluntarily dislocate the shoulder are poor surgical candidates;
surgery is rarely successful for them.
 |
|
|
|
Use the buttons above to see the different steps.
|
| |
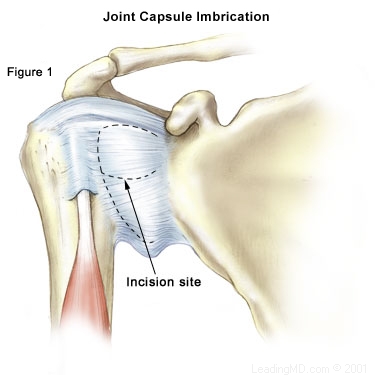
Traditional Approach
The traditional surgery for MDI is designed to make the joint capsule
smaller and reduce glenohumeral movement. This open surgical procedure
is called an extensive inferior capsular release and imbrication.
- The lower portion of the joint capsule is cut and overlapped
to tighten the ligaments and make the capsule smaller.
- During this procedure, the subscapularis muscle is detached
so the surgeon can access the joint capsule. It is reattached
at the end of the procedure.
- The success rate of this procedure is about 75% in a group
of carefully selected individuals (those who were determined
to be good surgical candidates after a careful history and examination).
Since there can be a substantial loss of motion with this
procedure, athletes may not be able to return to competition
after surgery.
Arthroscopic Techniques
Recently, new arthroscopic techniques have been developed to correct
multidirectional instability.
- Capsular plication (a pleating and stitching
technique) uses arthroscopic sutures to reduce the size of the
joint capsule.
- Thermal capsulorrhaphy is a technique that uses
thermal energy to shrink the capsule. This method is being evaluated
and looks promising, as it is less invasive and may reduce loss
of motion.
These arthroscopic techniques are very exciting, but remain experimental,
especially for athletes who require stability and the preservation
of motion.
What types of complications may occur?
The most common complication is recurrent instability, which can
happen in 20% or more cases, even with carefully chosen patients.
Post-operative stiffness and loss of motion are also complications;
however, loss of motion is often an acceptable result of achieving
stability. An average loss of motion in external rotation is about
10 degrees. A loss of motion greater than that occurs in about 5%
of the cases. Other small risks (less than 1%) common to most surgery
procedures include infection, nerve damage, or blood vessel injury.
|
 
© 2015 by LeadingMD.com All rights reserved.
Disclaimer
|
| |
|
Stem cells, PRP, and HA, oh my! We are not in Kansas anymore
Part 2
READ MORE >>
|
|
|
|